Hindfoot Valgus in Children: Does the Tilted Heel Self-Correct?
Heel tilted inward, often together with flatfoot. Seek evaluation if rigid or painful. Pediatric orthopaedic assessment Milan.
Quick Answers
Is hindfoot valgus the same as flatfoot?
When should hindfoot valgus be a concern?
Are orthotics needed for hindfoot valgus?
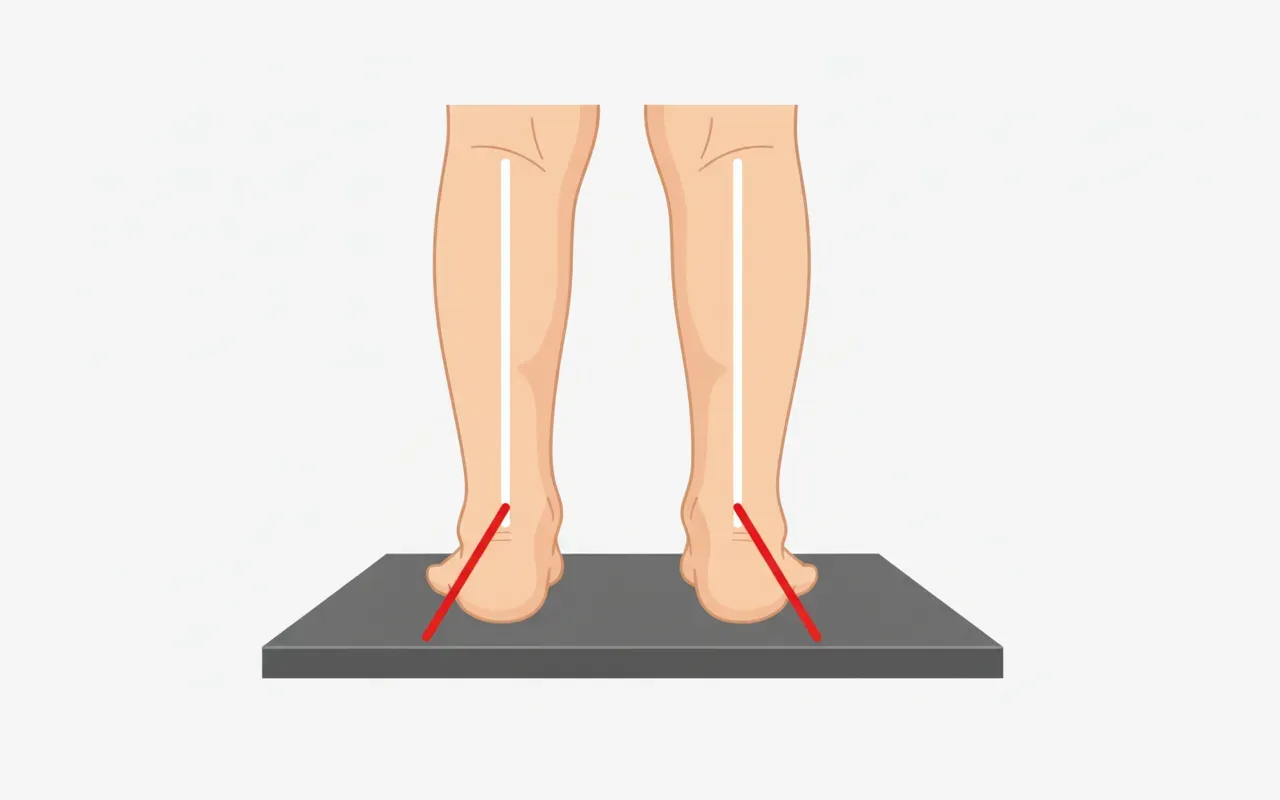
Hindfoot valgus is the condition in which the heel, viewed from behind, appears tilted inward relative to the leg axis. It is almost always associated with flatfoot and is part of the same overall pattern of foot pronation in weight-bearing.
In the great majority of children it is a physiological posture: calcaneal valgus peaks around 2-4 years of age and then progressively reduces as the plantar arch develops and the stabilising muscles mature. It becomes a concern when it is particularly marked, asymmetric between the two sides, rigid (does not correct with manipulation or on tip-toe standing) or associated with pain.
Clinical assessment is central: I measure the hindfoot angle in weight-bearing, check subtalar mobility, look for Achilles tendon tightness and — crucially — rule out tarsal coalition, the main cause of rigid hindfoot valgus in adolescents. Treatment is conservative in most cases (observation, orthotics, physiotherapy); surgery is reserved for severe symptomatic cases.
When to seek evaluation
- Marked or asymmetric hindfoot valgus
- Foot or ankle pain
- Fatigue during prolonged walking
- Asymmetric shoe wear
- Rigid hindfoot valgus
What is evaluated
- Weight-bearing hindfoot angle
- Subtalar mobility
- Correlation with flatfoot
- Foot X-rays when indicated
- Exclusion of tarsal coalition
Treatment options
- Observation in physiological cases
- Corrective orthotics in symptomatic cases
- Physiotherapy for muscle strengthening
- Arthroereisis or corrective surgery in selected cases
When Surgery Is Needed
Frequently Asked Questions
Is hindfoot valgus the same as flatfoot?▼
When should hindfoot valgus be a concern?▼
Are orthotics needed for hindfoot valgus?▼
Important Notice: The information on this page is for educational and informational purposes only and does not constitute medical advice. Each clinical case is unique: the appropriate treatment is determined during the specialist consultation, based on a thorough clinical examination and, where necessary, diagnostic imaging. For any doubts or concerns, please consult a specialist.
Learn more
Related Articles

Flatfoot in children: are orthotics really necessary? (and when they are)

Blount's Disease: Recent Literature Review and Treatment Strategies

Medial Epicondyle Fracture in Children: Cast or Surgery? Why Measuring Millimeters Isn't Enough
Email: daniele.priano@ortopediaevolutiva.com
Related conditions
- FootFlatfoot in Children: When to Worry
- FootTarsal Coalition: Painful Rigid Flatfoot in Adolescents
- FootJuvenile Hallux Valgus: Evaluation and Treatment
- GrowthKnock-knees and Bow legs: Crooked Legs in Children
Medical Glossary
Don't understand a medical term? Check our glossary with simple explanations.
Open glossary →